









Recently, blood flow restriction (BFR) training has been discussed more and more in the fitness, sports, and rehabilitation worlds. Growing evidence has continued to show its potential to improve exercise and rehabilitation programs. By intermittently restricting blood flow during exercise, the research supports significant ability to make gains in strength, muscle size, endurance and even injury recovery – often within abbreviated timetables. But what exactly is BFR and is it something that you should consider? How does it work? Is it safe? Is it effective? What are the best ways to utilize BFR?

First we need a brief description of how exercise works in the body
- The body needs to get oxygen to working muscles (or they will stop working)
- This occurs by moving blood to the muscles - the muscles extract oxygen from the blood and place it into the muscle tissue
- When these muscles are used, by repeating the contraction of specific motor units, they “fatigue”
- “Fatigue” is felt when the body's baseline of normal (or homeostasis) in the working tissues is disturbed
- The disturbance associated with “fatigue” signals both local and systemic responses...Basically, your body is attempting to respond to this stress. It does so in order to allow the motor units to sustain the activity (exercise) you are asking it to complete
- In the case of exercise under restricted blood flow conditions, this disturbance is caused by strong, but not complete, hypoxia - which creates a decrease in intracellular phosphate stores (ATP/PC)
Here are the steps of how this process works LOCALLY:
Step 1: Occlude venous outflow, while maintaining arterial inflow (this is an important safety element)
Step 2a: Apply easy exercise on muscles whose blood flow is restricted
- With “easy" exercise, contraction of most easily recruited motor units, fire first
- These motor unit contractions use the available intracellular phosphates (ATP/CP)
- Decreases in these phosphates, along with increases in "waste" (think Lactate) occurs in these exercising motor units
- As these first recruited fibers begin to fail, other motor units need to be recruited to take over providing the force to perform the exercise
- A disturbance of homeostasis or “metabolic crisis” ensues
Step 2b: Activate to achieve a muscle pump
- As exercise is performed, motor units contract, which squeezes blood out of the muscle
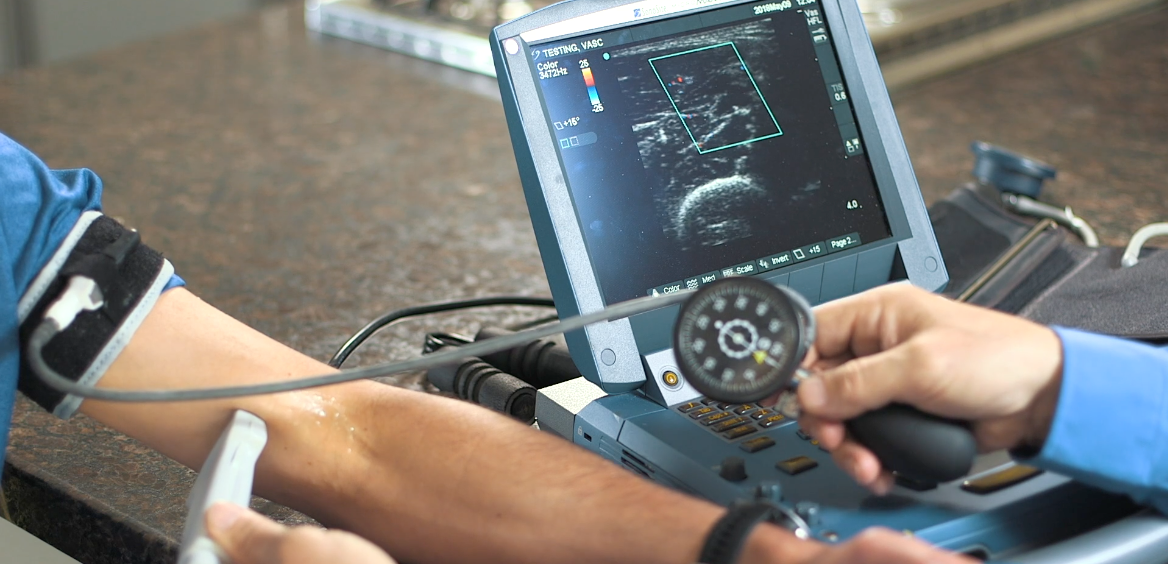
- With muscle contraction, blood is “pumped” from the distended extremity, out the deep veins and the open artery (documented by Doppler of retrograde flow in the artery)
- With this contraction, a large pulse of venous blood moves past the venous blockade (created by the BFR band) back into the central circulation...veins have valves that prevent blood flow back into the exercising muscle
- The arteries do not have valves, so as the muscle contraction relaxes, arterial blood rapidly fills in the now emptied peripheral vasculature and muscle space
- In this way, the blood flow to working muscle is increased and O2 is still being delivered
- So on one hand, the exercise creates more of a deficit of O2, as well as a greater demand of O2…but the muscle pump still allows for the delivery of blood and O2 to working muscle, albeit an overall significant decrease than at a normal state because the blood flow is restricted
Step 3: A Disturbance of Homeostasis
- A cascade of “failure” begins throughout the muscle to a point where all motor units have become fatigued and exhausted
- During rest intervals between sets and reps, blood flow remains restricted - because the bands are still on
- When exercise starts up again, the active motor units must function in an already “Disturbed Environment” resulting in recruitment of most, if not all motor units to perform the exercise
- Recruitment of additional motor units, also ultimately fatigue until “failure”
- Thus, BFR is facilitating recruitment, utilization and fatigue of working motor units (similar to any exercise), but it is able to do so with a much less overall loading/intensity - research would indicate as low as 30% of one's 1 repetition maximum.
First we need a brief description of how exercise works in the body
- The body needs to get oxygen to working muscles (or they will stop working)
- This occurs by moving blood to the muscles - the muscles extract oxygen from the blood and place it into the muscle tissue
- When these muscles are used, by repeating the contraction of specific motor units, they “fatigue”
- “Fatigue” is felt when the body's baseline of normal (or homeostasis) in the working tissues is disturbed
- The disturbance associated with “fatigue” signals both local and systemic responses...Basically, your body is attempting to respond to this stress. It does so in order to allow the motor units to sustain the activity (exercise) you are asking it to complete
- In the case of exercise under restricted blood flow conditions, this disturbance is caused by strong, but not complete, hypoxia - which creates a decrease in intracellular phosphate stores (ATP/PC)
Here are the steps of how this process works LOCALLY:
Step 1: Occlude venous outflow, while maintaining arterial inflow (this is an important safety element)
Step 2a: Apply easy exercise on muscles whose blood flow is restricted
- With “easy" exercise, contraction of most easily recruited motor units, fire first
- These motor unit contractions use the available intracellular phosphates (ATP/CP)
- Decreases in these phosphates, along with increases in "waste" (think Lactate) occurs in these exercising motor units
- As these first recruited fibers begin to fail, other motor units need to be recruited to take over providing the force to perform the exercise
- A disturbance of homeostasis or “metabolic crisis” ensues
Step 2b: Activate to achieve a muscle pump
- As exercise is performed, motor units contract, which squeezes blood out of the muscle
- With muscle contraction, blood is “pumped” from the distended extremity, out the deep veins and the open artery (documented by Doppler of retrograde flow in the artery)
- With this contraction, a large pulse of venous blood moves past the venous blockade (created by the BFR band) back into the central circulation...veins have valves that prevent blood flow back into the exercising muscle
- The arteries do not have valves, so as the muscle contraction relaxes, arterial blood rapidly fills in the now emptied peripheral vasculature and muscle space
- In this way, the blood flow to working muscle is increased and O2 is still being delivered
- So on one hand, the exercise creates more of a deficit of O2, as well as a greater demand of O2…but the muscle pump still allows for the delivery of blood and O2 to working muscle, albeit an overall significant decrease than at a normal state because the blood flow is restricted
Step 3: A Disturbance of Homeostasis
- A cascade of “failure” begins throughout the muscle to a point where all motor units have become fatigued and exhausted
- During rest intervals between sets and reps, blood flow remains restricted - because the bands are still on
- When exercise starts up again, the active motor units must function in an already “Disturbed Environment” resulting in recruitment of most, if not all motor units to perform the exercise
- Recruitment of additional motor units, also ultimately fatigue until “failure”
- Thus, BFR is facilitating recruitment, utilization and fatigue of working motor units (similar to any exercise), but it is able to do so with a much less overall loading/intensity - research would indicate as low as 30% of one's 1 repetition maximum.
If your muscles and tendons are only being stressed at light loads of 30% of their ability, but achieving the benefit of training like that of more then double the forces, it is easy to see how this could be a highly effective training tool in the rehab, fitness and sports performance worlds!
Now, let's talk about the mechanism(s) of how exercise & BFR works SYSTEMICALLY:
- Your central nervous system (brain and spinal cord) also registers the metabolic "crisis" from exercises with blood flow restricted - so, it sends out signals to compensate
- Your autonomic nervous system (fight or flight) reacts by increasing sympathetic tone, heart rate, ventilation and sweating (all of which is out of proportion to the actual work being done by the muscle)
-
Hormones involved in repair processes are also triggered, and released throughout your body.
- Hormones such as human growth hormone (HGH) and insulin-like growth factor (IGF) are among two of the most prominent ones...Yes, you are stimulating the release of HGH!
- Systemically, research has shown muscle growth/strength/endurance that occurs both on the distal and proximal sides of the band…for example, while you're only restricting blood flow to your arms, your pecs are also affected and encouraged to increase in mass/strength/endurance.
- Also, because your vasculature is made up of smooth muscles and they are also "working out", research has shown an ability to actually improve one's vascular health with BFR, too
1. LIGHT WEIGHTS + BFR PRODUCES PROFOUND MUSCLE FATIGUE (LOCALLY)
2. NERVOUS SYSTEM COMMUNICATES FEELINGS OF FATIGUE TO BRAIN (SYSTEMICALLY)
3. BRAIN RELEASES GROWTH HORMONE
4. HORMONES CIRCULATE IN BLOOD STREAM
5. HORMONE RELEASE FACILITATES REPAIR AND INCREASE STRENGTH IN ALL EXERCISED TISSUES...INCLUDING DISTAL AND PROXIMAL TO THE BFR BANDS
(This is an oversimplification of the complex theory of the mechanism behind BFR, but it addresses the basics mechanics of what is happening in the body)
SOURCES
Credit: Joel Novak at My Performance Rehab
- Loenneke JP, Wilson JM, Marín PJ, Zourdos MC, Bemben MG (2012). Low intensity blood flow restriction training: a meta-analysis. European Journal of Applied Physiology, 112(5), 1849-1859.
- Slysz J, Stultz J, Burr, JF (2016). The efficacy of blood flow restricted exercise: A systematic review & meta-analysis. Journal of Science and Medicine in Sport, 19; 669–675.
- Anderson M, Lance L (2017) Blood Flow Restriction Therapy: Theories, Science, and Current Clinical Results. Newsletter of the AOSSM, Spring 2017; 2-6.
- Hughes L, Paton B, Rosenblatt B, Gissane C, Patterson DP (2017). Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. British Journal of Sports Medicine, Jul;51(13):1003-1011.
- Horiuchi M, Okita K (2012). Blood flow restricted exercise and vascular function. International Journal of Vascular Medicine, 2012:543218.
- Manini, TM, Yarrow JF, Buford TW, Clark BC, Conover CF, Borst SE. Growth hormone responses to acute resistance exercise with vascular restriction in young and old men. Growth hormone and IGF Research. Oct;22(5):167-72.
- Fry CS, Glynn EL, Drummond MJ, Timmerman KL, Fujita S, Abe T, Dhanani S, Volpi E, Rasmussen BB (1985). Blood flow restriction exercise stimulates mTORC1 signaling and muscle protein synthesis in older men. Journal of Applied Physiology, May;108(5):1199-209.
- Heitkamp HC (2015). Training with blood flow restriction. Mechanisms, gain in strength and safety. Journal of Sports Medicine and Physical Fitness, May;55(5):446-56.
- Shimizu R, et al (2016). Low-intensity resistance training with blood flow restriction improves vascular endothelial function and peripheral blood circulation in healthy elderly people. European Journal of Applied Physiology, Apr;116(4):749-57.